It was a cruel stroke of fate that abruptly ended Mike Firth's underwater adventures, but this UK diver is keen that his misfortune should serve as a warning to anyone tempted to skimp on kit hygiene.
STEVE WEINMAN reports
IN LATE 2008, DIVER received several phone calls from a clearly agitated diver. He was desperate to find someone – anyone – who could explain what was wrong with him.
We offered a few ideas about medical specialists he might contact, and wondered what the outcome would be.
Now we know. Mike Firth is a housebound invalid, waiting for a lung transplant, and his life changed because he took two deep breaths off his wing.

Mike, a diver since his early teens, says he was a very fit 56-year-old. A deep-air diver but trimix-trained, he says: “I was happiest diving Bridlington Bay in East Yorkshire at 40m maximum, using my ABLJ and on nitrox,” he says.
“More-time-less-deco suited me fine, but my buddies and I dived previously undived wrecks, so we sometimes had to go deeper, using hi-tech equipment. Care and attention to detail was required, whether we were using rebreathers or on open-circuit.”
In 2008, Mike toured South America, Cocos and Cuba, in part pursuing his interest in marine biology. He returned to the UK in November, looking forward to a new career as a marine biologist, and resumed his diving in the North Sea.
Following some 50m-plus dives, Mike began suffering intermittent raised temperatures, shaking, dry hacking coughs and lethargy.
Soon he couldn't breathe easily while standing, or even sitting, for any length of time. Accustomed to walking miles each day, he would now grow short of breath within 25 metres.
His GP took blood samples, but they showed no abnormalities. Mike then approached his local diving specialist, and the Diving Diseases Research Centre in Plymouth. X-rays revealing a “shadow” precipitated a move to hospital in Leeds. He would be hospitalized for the next 10 months.
THE FIRST THREE WEEKS Mike spent in intensive care, mostly sedated, with tracheotomy and intubation.
He says that he was experiencing “interesting” hallucinations, and shed 30kg in that time.
There was still no firm diagnosis, but there were indications that he was showing signs of responding to anti-fungal drugs, and sputum samples revealed signs of the fungus aspergillus. That's when Mike started to wonder about his wing.
Both he and his wife mentioned their suspicions to staff, but he says they were not followed up. “I was hours from death twice, and told by my consultant on another two occasions that I was dying – but hell no, divers revert to training and survive,” he says.
“I was going from crisis to crisis, and the medics were getting nowhere. I was too ill to speak at times, and my wife wasn't being listened to. We tried to tell everyone my dive kit needed testing.”
As soon as Mike was able to do so, he called on diving buddies and contacts around the world for advice. It was around this time that he called DIVER.
In May 2009, he was pointed to the recently opened National Aspergillosis Centre (NAC) at Manchester Wythameshaw Hospital. And within a week of referring himself there, his kit had been tested and a diagnosis made.
Mike was told that he had developed a fungal infection of the lungs caused by contaminated diving equipment.
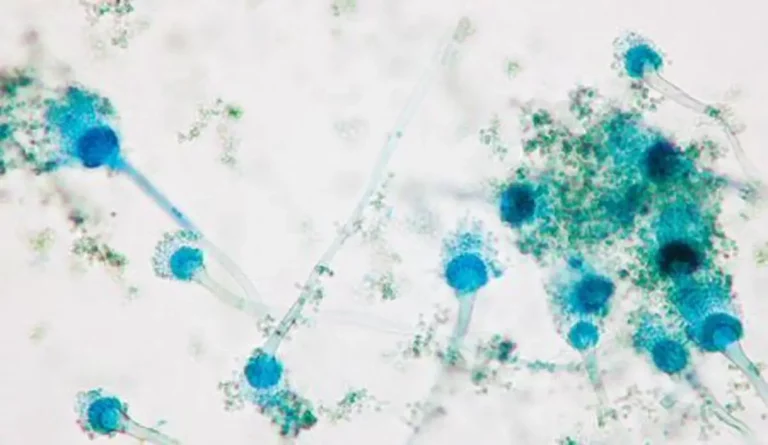
The culprit was Aspergillus fumigatus, a micro-organism that exists within all our bodies, and in the air, but usually safely contained by our immune systems.
“In my case it decided to take over my entire lung system, and that first December I had been closer to death than most cats,” says Mike.
Worldwide, aspergillus causes millions of allergic and chronic infections. The number of cases
has risen steadily with increasing recognition, until today it is the most common invasive mould infection, according to the NAC.

But Mike had a more acute form called invasive aspergillosis. Death is virtually guaranteed if the disease is left untreated, and fatality remains as high as 40-90% even with treatment.
SO HOW DOES MIKE think it started? “I remember a post-dive inspection on which I had cleaned all my kit and dried it externally,” he says. “I drained residual internal air and water from my wing via the dump valves.
“The last thing I did was ensure that the manual inflator was working, both in and out. I took two deep breaths, and there was a taste of mould when I breathed in.
“I immediately washed the inner bag out with Milton [sterilizing fluid], which I have used for years. I never breathed from the inflator again.”

The tests on his wing, only ever used in the North Sea, proved it to be “riddled with fungus, especially on the hard black plastic within the sealed-bag system, corrugated tubing and mouthpiece”.
His other kit, including his BC for pool training and ABLJ for depths up to 40m, was given the all-clear.
As an experienced technical diver, Mike maintains that he never skimped on pre- and post-dive maintenance.
“Whatever my kit needed, it got,” he says. “I probably looked after it better than I did my wife.
“My wings had never given me any problems since purchase. I'd never used them for anything other than buoyancy. I dived using multiple redundancy.
“Cylinders were pristine, and I used only one compressor. Regulators [all seven of them] were untainted.
I'm an old-school diver, trained the old BSAC way on a Fenzy Mk 1 ABLJ.
If you were unable to breathe from that for a set period, you weren't allowed to dive.”
When Mike Firth first suspected that his infection was diving-related, he contacted several manufacturers of closed-bag BCs and wings to ask if they were aware of anything having grown inside them. Salt crystals apart, they told him, no such thing had occurred.
“I didn't believe them then, and I don't now,” says Mike. “All my friends in the UK use Milton to rinse their BCs, and those with rebreathers use the prescribed cleaning brand.”

Mike believes his affliction sounds a warning to the diving community.
“I would suggest that no divers should breathe from the manual inflation device of their BC in any way, because of the danger of breathing in this devastating fungus,” he says.
“And the manufacturers might like to tweak their user guidelines for maintaining cleanliness, before a nanny-state department does it for them.”
DIVERS KNOW THAT IN an out-of-air emergency there is always the possibility of draining any air remaining in the BC through the inflator mouthpiece. Training agencies don't teach this technique, however, because of the possibility of respiratory infection.
The counter-argument has always been that risking lung infection is better than dying from lack of air, and that disinfecting a BC removes the risk of infection anyway. But does it?
Professor of Mycology David Denning, Director of the National Aspergillosis Centre, says that Mike Firth's is the only diving-related case he has come across, and that more research is needed into why his body reacted as it did.
“Aspergillus infections in divers may be more common than we think,” he says. “What was unusual in this case was what we did, which was to take his kit apart and culture it. No-one else would do that.
“His lung reaction was clearly very unusual, and you wouldn't normally expect such a very extreme clinical reaction in someone who's fit enough to dive. People with bad lungs, with TB or asthma or even bad sinusitis, might be expected to react in this way, but then, they wouldn't normally be diving.”
What about Mike's regular use of Milton as a sterilising agent? “Sodium hypochlorite [the active ingredient in Milton] is likely to have an impact on the aspergillus fungus, but it won't necessarily kill it,” says Prof Denning.
A new Health & Safety Executive information sheet, Cleaning of Diving Equipment, came out this August and is relevant not only to manufacturers but to recreational divers, says the HSE.
It provides guidance on minimising risks from micro-organisms that can be present in BCs as well as regulator mouthpieces, rebreathers and so on.
Diving equipment by nature, and the fact that it might be stored in a damp condition, creates an environment in which fungi, yeasts, bacteria and viruses can multiply rapidly, says the HSE.
“Fungi are one of the most likely contaminants, and these can produce large quantities of spores. Inhalation of these spores can cause an allergic reaction in the lungs, producing potentially life-threatening conditions, particularly in those individuals who may be predisposed to allergy,” it states.
The given solution is to thoroughly clean and dry equipment, particularly those parts that might allow a direct path to your lungs
After a day's diving, the minimum recommended cleaning regime is thorough rinsing of these surfaces with clean drinkable water, to flush away any minute deposits that could act as nutrients for microbial growth, followed by complete drying.
If water quality is in doubt, use sterile, boiled or bottled water for rinsing.
As the microbial agents can be “opportunistic and tenacious”, periodic disinfection should also be considered, particularly of shared equipment.
The manufacturer's instructions should always be followed, but preferably the disinfectant used should be effective against the most resistant micro-organism – in this context, Mycobacterium tuberculosis (TB).
After drying, store in a dry, clean environment – ideally, an enclosed room with circulating air and minimum exposure to airborne contaminants. I asked Steve Field, HSE Specialist Diving Inspector, if more specific advice on a disinfectant would not be helpful.
“While it's important that the disinfectant used is effective and safe, it's also important that it doesn't damage the equipment,” he said.
“Manufacturers employ a wide range of materials in their products and they are therefore best-placed to advise on what disinfectant is compatible with the materials they use.”
And as the guidelines make clear, manufacturers' instructions must be followed carefully, because inhaling unrinsed disinfectant can itself pose a health hazard.
Incidentally, if you use a combined octo-inflator such as an AP Valves Auto Air or Scubapro Air Two, you inhale gas directly from your tank, and breathe off your BC bag only if the tanked gas runs out, at which critical point most divers will have other things than lung infections on their minds.

“Invasive pulmonary aspergillosis is extremely unusual in people with no other history of lung problems or altered immune system – diabetes, steroids, chemotherapy, HIV etc,” says diving doctor Ian Sibley-Calder.
“I've heard of the risks regarding inhaling from buoyancy devices, but have never seen or heard of a patient before.
“Consider the number of divers over the world and the fact that inhaling from a buoyancy device is relatively common – to extract air to collapse a wing, for instance, which I've done many times.
“While this case is tragic, and it's a fair point that we should all take care of our kit, I don't think we should be overly alarmist. If you need to breathe out of a buoyancy device because you've run out of air, do it. Be careful, but don't panic.”

THE PROGNOSIS FOR MIKE FIRTH is still dire. The prospect of having one or both lungs transplanted is complicated by the muscle-wasting, tiredness and breathing problems caused by his illness, and which stop him exercising.
With only 30% lung capacity, he requires oxygen round the clock: “It's like having your face blown away, and it makes my mouth and nose tissues very sore… I have to settle for being able to walk no more than about 15 metres, and my buddy is a long line with piped O2.
“I can no longer dive, which is very sad,” says Mike. “I can't pass on my skills to others as I have in the past.
I can't look down on long-lost wrecks in my North Sea, or those fun-dives like the Scylla, Cadmus or Pilsudski. My lungs have been trashed by this fungus.”
HSE Information Sheet 12, Cleaning of Diving Equipment.